
Skilled Nursing Care: Choosing the Right Path for Your Loved Ones
In an era where aging demographics are on the rise, understanding the variety of skilled nursing care options becomes paramount to provide the best solutions …
In an era where aging demographics are on the rise, understanding the variety of skilled nursing care options becomes paramount to provide the best solutions …

The treatment of obstructive sleep apnea with continuous positive airway pressure (CPAP) devices proves to be not only an effective method of symptom relief, but …

Choosing the right path for dental assistant training is crucial for aspiring dental professionals. With advancements in technology, online training programs have become increasingly popular. …

In today’s world, where health and fitness are paramount, many individuals are turning to technology to aid in their weight loss journey. One such technological …

Selecting the perfect haircut isn’t just about following the latest trends; it’s about finding what truly complements your unique face. Whether you’re aiming for a …

Life alert devices have become essential tools, especially for senior citizens, to attain home security. They can live a life of peace and confidence, and …

Singapore, a cosmopolitan city-state known for its towering skyscrapers, lush green parks, and a blend of cultures, stands as a beacon of modernity and efficiency. …

Cardiology has seen a revolution because of advancements in cardiovascular imaging tools, which have given medical professionals a new perspective on the anatomy and physiology …

In the tricky world of health and taking pills daily, keeping track of many prescriptions can be a big headache, especially for people dealing with …

In the world of fixing teeth, dental implants are like the superheroes. They’re not just there to fill the gap. They make sure you keep …

Good nutrition is the cornerstone of a healthy life at every stage. However, nutritional needs evolve as we pass through different life stages, each with …
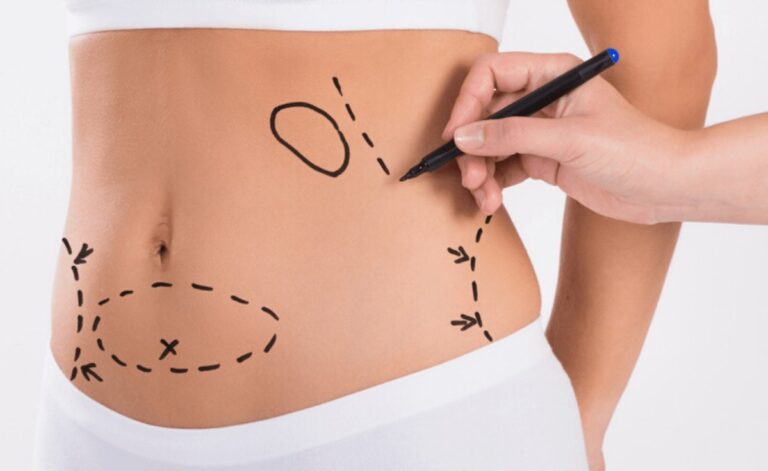
Liposuction is a highly effective, non-invasive cosmetic procedure incorporated for reducing accumulated body fat from areas such as the stomach, hips, thighs, neck, arms, etc. …

Anemia, a condition marked by a deficiency of red blood cells or hemoglobin, affects millions of people worldwide, leading to fatigue, weakness, and other health …

Remember that first win? It felt good, right? Like, really good. So, you think to yourself, “I’ll just try one more time. What’s the harm?” …

Moving to Singapore presents an exciting opportunity for expats, but it also requires careful consideration of health-related matters. This blog post offers insights into navigating …
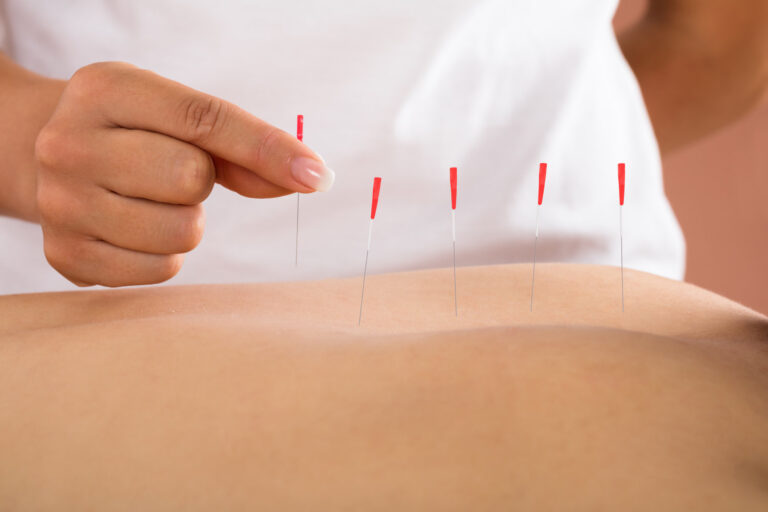
A type of physical therapy called dry needling is becoming increasingly well-liked as a successful means of treating pain and accelerating the healing of injuries. …

Dental implants have completely changed the field of dentistry by providing people with a dependable, long-term tooth replacement. When it comes to restoring smiles, dental …

A staple of the Mediterranean diet, extra virgin olive oil is recognized for its many health advantages in addition to its many culinary applications. This …

When living with celiac disease, the focus often lands squarely on the digestive disturbances it causes. Yet, there’s a less visible but equally challenging symptom that …

For ages, reflexology has been utilized as a traditional medicine to address a range of ailments. Does reflexology, however, function? And what’s the science involved …

Derived from the seeds of the hemp plant, this oil has been gaining popularity in the culinary world for its nutty flavor and numerous health …

Understanding and addressing the mental health challenges faced by teenagers is of utmost importance in today’s world. Adolescents today face an unprecedented and constantly evolving …

In the realm of healthcare, the debate between conventional and alternative medicine often sparks intense discussions. While some individuals swear by the efficacy of alternative …
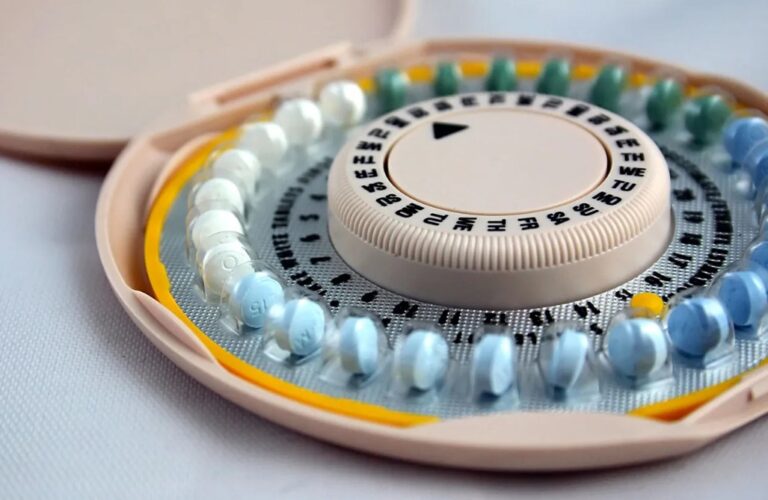
Birth control pills are a straightforward, easy, and safe method of preventing pregnancy. Further, it lessens menstrual cramps, lightens and regularizes your periods, and lessens …

Tennis elbow, a common condition characterized by elbow pain, often puzzles those who suffer from it. This condition, while not life-threatening, can significantly impact daily …

In recent years, there has been a growing concern about the rising prevalence of depression and mental health challenges among adolescents. Although the reasons are …

In recent years, Turkey has emerged as a prominent destination for health tourism, attracting individuals from around the world seeking high-quality medical treatments and wellness …

Celiac disease, a chronic autoimmune disorder triggered by the ingestion of gluten, affects millions of Americans every day. As individuals grapple with the challenges of …
The field of ophthalmology has seen remarkable advances over the past few decades, from new diagnostic technologies to innovative surgical techniques. These advancements have propelled …